Fertility care generates more clinical data per patient than almost any other medical speciality and most of it is still being documented by hand. For clinics running five or more consultations a day, that manual effort quietly consumes hours that belong to patients. AI medical scribe for IVF clinics technology changes that equation by capturing, structuring, and delivering clinical notes in real time, without disrupting how your team works.
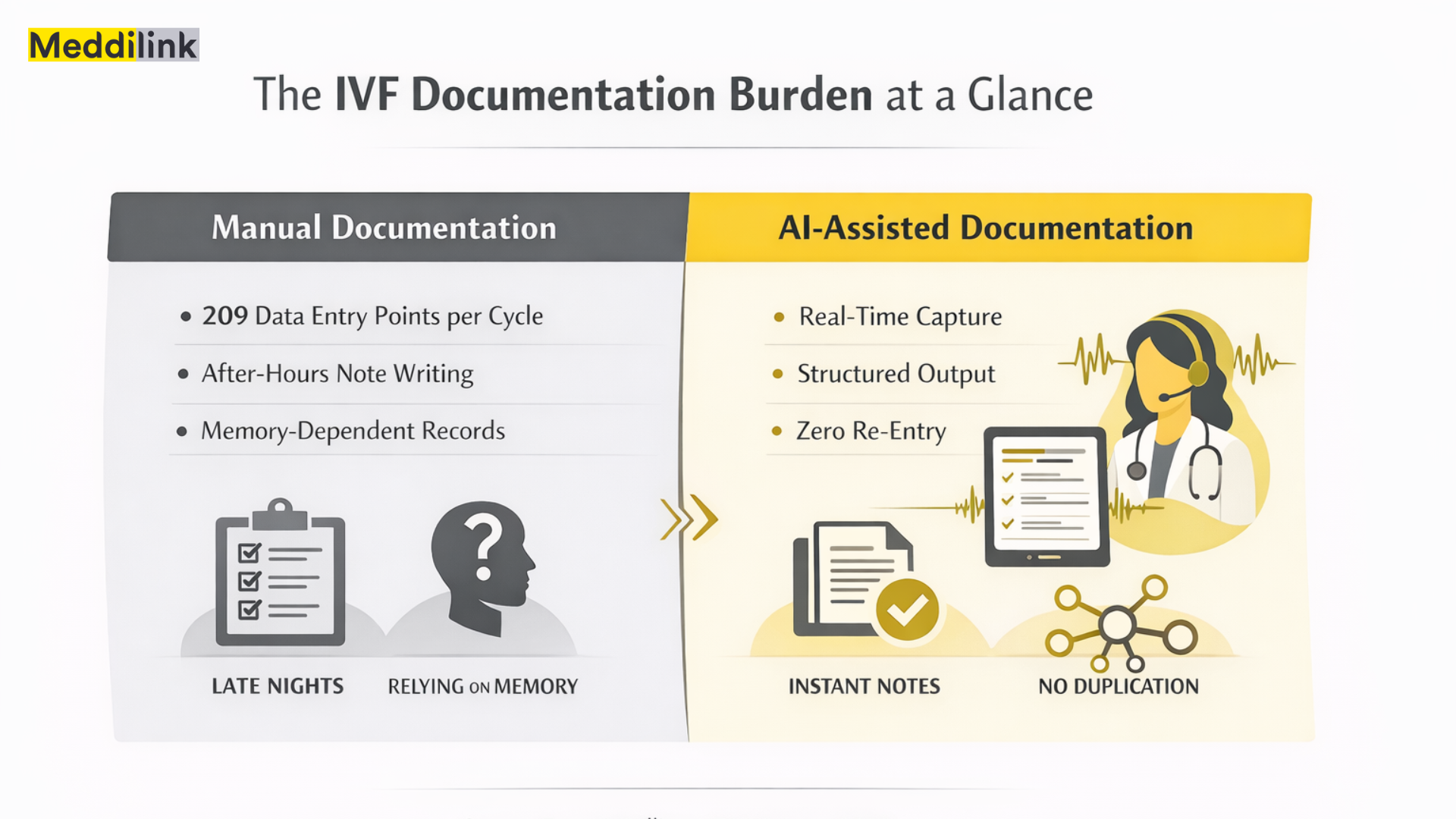
A 2023 study in F&S Sciencefound disconnected IVF documentation systems required an average of 209 manual data entry points per treatment cycle. Even clinics using integrated digital tools averaged 18 entry points per cycle. The automation gap is clear, and automated EMR documentation is how leading fertility clinics are closing it.
This article explains the problem, what the evidence says about AI scribes, and how MedAI Scribe addresses the specific demands of IVF workflows.
The Hidden Cost of Manual IVF Documentation
Ask most clinic managers how documentation is going, and they will say it is fine. What they mean is that notes eventually get written. What they may not be tracking is how long that takes, when it happens, and what the team pays in attention and energy to make it happen.
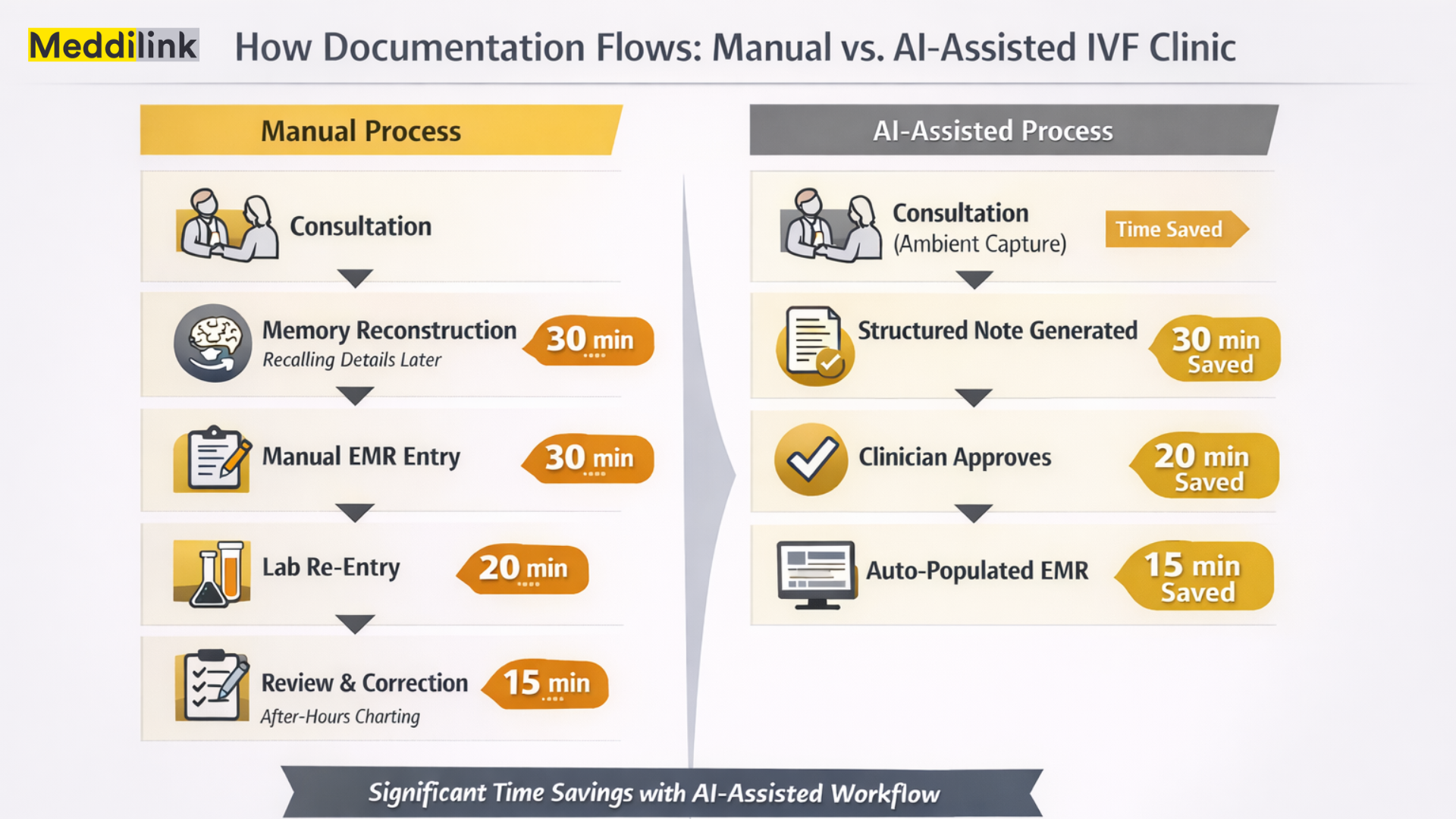
AMA data from 2024 showed that for every eight hours physicians spend with patients, they spend five or more hours on the EHR. A significant share of that happens after hours, which the AMA calls “pajama time.” Across a fertility team of five clinicians, that is a potential 50+ hours of recoverable capacity every week.
In IVF, the complexity compounds this further. Embryologists grade embryos and transcribe findings into separate systems. Fertility doctors conduct monitoring consultations and reconstruct details from memory afterwards. Clinical and lab teams share data across platforms that frequently do not talk to each other, creating duplicate entry and reconciliation loops.
The documentation gets done. But it costs the team more than any workflow audit tends to capture.
The real cost: not just time
Notes written from memory two hours after a consultation are less complete than notes captured in real time. Less complete records create coordination gaps between clinical and lab teams. Those gaps affect cycle decisions. For clinics competing on outcomes, this chain matters.
Why Standard EMRs Don’t Solve the Problem
Electronic medical records improved data storage and accessibility. They did not reduce the effort required to create that data.
IVF workflows demand more from a documentation system than any standard EMR was designed to handle: partner-linked records, cycle-stage sequencing, embryo development tracking, and dual documentation across clinical and lab functions. Standard EMRs accommodate general clinical patterns. IVF is not general.
Dedicated fertility EMRs have narrowed this gap, but manual input remains the norm. The F&S Science study makes this concrete: clinics on integrated platforms still averaged 18 manual entry points per cycle. The digitisation happened. The clinical documentation automation IVF teams actually need did not.
What the Evidence Says About AI Medical Transcription in Clinical Settings
Real-world data on AI scribes is now substantial enough to take seriously. A year-long evaluation at The Permanente Medical Group (Kaiser Permanente), published in NEJM Catalyst in 2024, tracked 7,260 physicians across 2.5 million patient encounters. AI scribe use saved an estimated 15,791 hours of documentation time and was associated with measurable reductions in after-hours documentation and clinician burnout.
A separate randomised controlled trial at UCLA Health, published in NEJM AI in 2025, found a 10% reduction in documentation time per note across 238 physicians and more than 72,000 encounters.
These studies were conducted in primary care and general outpatient settings. IVF-specific data have not yet been published in peer-reviewed literature. But the documentation challenge in fertility care is measurably more complex than in primary care; the potential benefit is at least comparable.
On accuracy: what the data shows
Kaiser Permanente’s pilot evaluated 35 AI-generated transcripts, scoring them an average of 48 out of 50 on accuracy, consistency, lack of bias, and succinctness. In MedAI Scribe, every note is reviewed and approved by the clinician before it enters the patient record. The AI drafts. The clinician decides. Source: NEJM Catalyst, 2024.
Why IVF Clinics Cannot Use Generic AI Note Taking for Doctors
Most AI documentation tools available today were built for primary care. They handle general clinical vocabulary well. They do not handle IVF-specific documentation needs:
- Embryo grading: Notation follows specialised morphological systems, Gardner, Veeck, and Istanbul consensus that general clinical AI will not recognise or correctly structure.
- Stimulation monitoring: The same hormone value carries different clinical weight on day three versus day eight of stimulation. Context-free transcription misses this entirely.
- Partner-linked records: IVF requires dual-patient documentation logic that single-patient templates cannot support.
- Lab-to-clinic handoffs: Structured data transfer between embryology and clinical records requires format alignment that generic tools do not generate.
- Regulatory documentation: Consent records, genetic testing logs, and cryopreservation documentation each carry compliance requirements that a general AI note-taker will not capture.
Clinical documentation automation IVF requires a system built with fertility clinical logic as its foundation, not a general tool adapted after the fact.
How MedAI Scribe Works Within the Meddilink Platform
MedAI Scribe is Meddilink’s AI medical scribe for IVF clinics, built as the documentation layer of MedART, Meddilink’s broader IVF clinic management platform. It is not a standalone transcription tool bolted onto your existing EMR. It operates within a system already structured around IVF workflows.
In practice:
- Consultations are captured via ambient AI medical transcription, with no additional hardware, and no change to how clinicians work
- Notes are generated with IVF cycle context already embedded: the system knows which stage of treatment the patient is in and formats accordingly
- Output follows IVF clinical standards: SOAP notes, monitoring updates, embryology observation formats
- Records enter the MedART patient file directly, no re-entry, no reconciliation, no manual transfer
- Clinical and embryology documentation sit within the same data environment, reducing coordination gaps between teams
Because MedAI Scribe operates within MedART, the documentation data it generates feeds into the broader patient record, supporting cycle decision-making, audit readiness, and the structured data foundation that future AI tools in reproductive medicine will require.
Want to see this in your clinic’s workflow?
We run 30-minute walkthroughs for fertility clinic teams using real IVF cycle scenarios, not generic demos. You will see exactly how consultation notes, monitoring updates, and embryology records are generated and approved. Book at meddilink.com/demo, no commitment required. 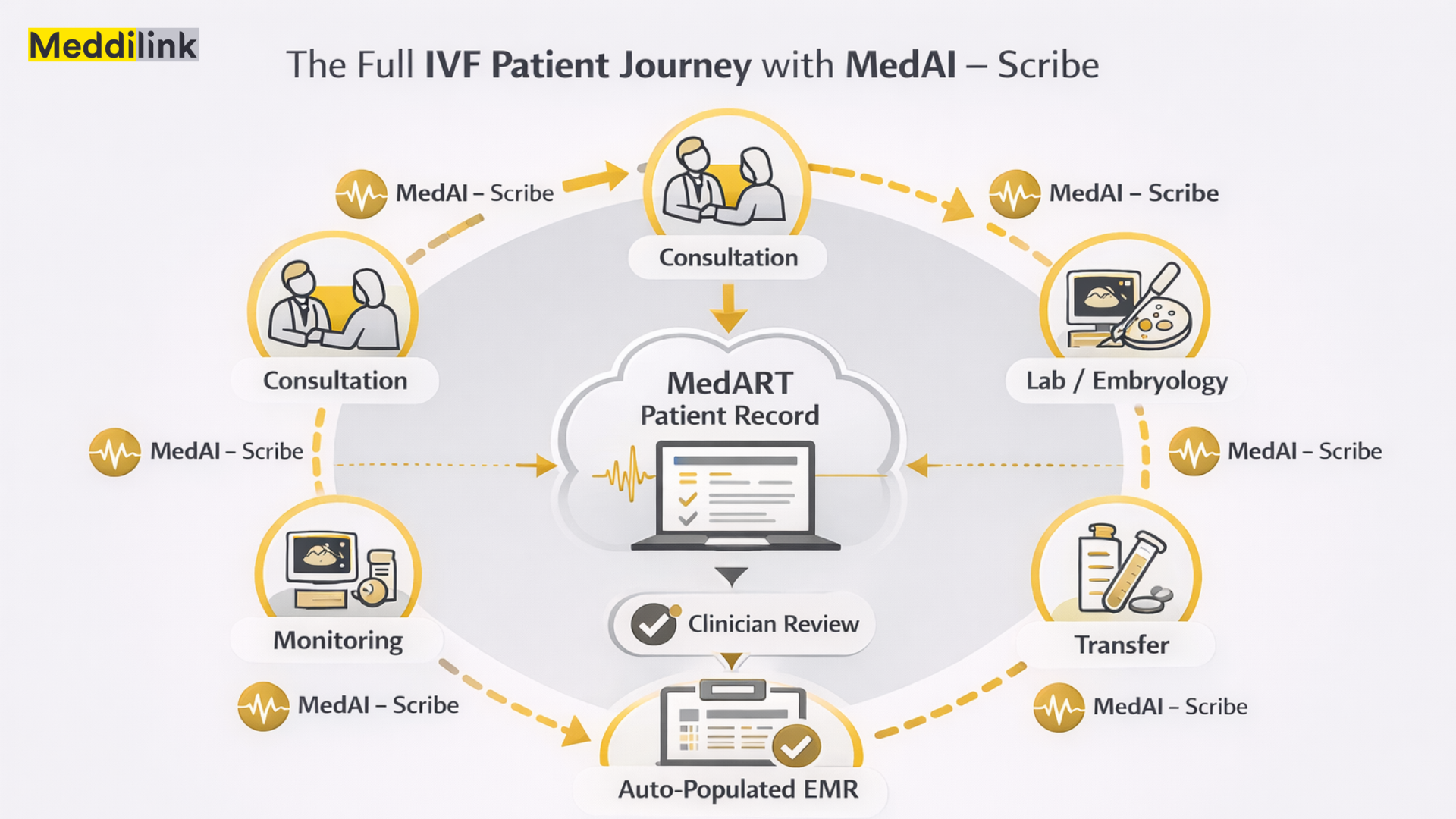
The Longer-Term Advantage: Structured Clinical Data
When documentation is automated and consistent across every clinician and every consultation, clinics accumulate something manual processes cannot produce: a high-quality, structured dataset across their entire patient population.
That dataset enables:
- Pattern recognition across cycles, identifying which stimulation protocols produce better outcomes for specific patient profiles
- More accurate benchmarking against your own historical data, not just published population averages
- Regulatory audit readiness by default, not by retrospective correction
- The data foundation for AI-assisted clinical decision support, the direction IVF technology is moving
Clinics building this foundation now will be better positioned as AI capabilities in reproductive medicine continue to develop. Those managing documentation manually will be working to catch up.
The Shift Is Already Underway
The documentation burden in IVF is not new. What is new is that the volume is growing, more patients, stricter compliance requirements, higher expectations for clinical continuity, and a credible alternative to manual documentation now exists.
An AI medical scribe for IVF clinics removes the friction that makes documentation the most draining part of the clinical day: split attention during consultations, memory-dependent note reconstruction, and after-hours catch-up. What remains is a clinician who is fully present, a record that accurately reflects what happened, and a data foundation built for what comes next.